

Every year, millions of people across India receive a recommendation that changes the course of their cardiac care: “You need a coronary angiogram.” For many patients, this recommendation arrives after an abnormal TMT stress test, unexplained chest pain, or a suspected heart attack. Yet despite being one of the most commonly performed cardiac procedures in the world, the coronary angiogram remains widely misunderstood — often feared because of unfamiliarity rather than genuine risk.
This comprehensive guide by Dr. T. Sandeep — Interventional Cardiologist at Jayam Hrudayalaya — demystifies the coronary angiogram completely. From what it is and why it is done, to the detailed step-by-step procedure, risks, recovery, and how results are interpreted, every question you have about a coronary angiogram is answered here.
What is a Coronary Angiogram?
Coronary angiogram what is it — this is the most fundamental question, and the answer begins with understanding what coronary arteries are and why they matter.
Your heart muscle is one of the hardest-working tissues in your body. To sustain its relentless pumping — over 100,000 beats every day — the heart muscle itself requires a constant, uninterrupted supply of oxygenated blood. This supply is delivered by three major blood vessels that wrap around the surface of the heart, collectively called the coronary arteries: the Left Anterior Descending (LAD) artery, the Left Circumflex (LCX) artery, and the Right Coronary Artery (RCA).
A coronary angiogram is a specialised X-ray imaging procedure that directly visualises the interior of these coronary arteries using a contrast dye. It is performed in a cathlab (catheterisation laboratory) — a specially equipped procedural room with advanced X-ray imaging systems — and provides cardiologists with a live, high-definition roadmap of the coronary circulation, revealing any blockages, narrowings, or abnormalities with remarkable precision.
The coronary angiogram is considered the gold standard investigation for diagnosing coronary artery disease — the condition where fatty plaques narrow or block the coronary arteries, reducing blood flow to the heart muscle and causing chest pain, breathless, or heart attack.
Why is a Coronary Angiogram Needed? Understanding When is Angiogram Needed
Understanding when is angiogram needed is critical, because this procedure is not a routine screening test — it is a targeted, definitive investigation performed when there is a specific clinical reason to directly evaluate the coronary arteries.
Primary Indications for Coronary Angiogram:
1. Positive or Suspicious TMT Stress Test When a treadmill test reveals ST-segment changes suggesting myocardial ischemia, the coronary angiogram is the natural next step to confirm whether a significant blockage is responsible.
2. Acute Coronary Syndrome — Heart Attack or Unstable Angina In a heart attack (STEMI or NSTEMI), emergency coronary angiogram is performed immediately to identify the blocked artery and proceed directly to angioplasty to restore blood flow. Time is heart muscle — every minute of delay increases permanent damage.
3. Stable Angina Unresponsive to Medications Patients with exertional chest pain that persists despite optimal medical management require a coronary angiogram to determine whether intervention (angioplasty or bypass surgery) is more appropriate than continued medical treatment.
4. Abnormal Non-Invasive Tests Abnormal nuclear stress tests, stress echocardiography, or CT coronary angiography findings indicating significant ischemia or high-risk anatomy warrant direct coronary angiogram evaluation.
5. Pre-Operative Cardiac Assessment Certain high-risk patients require a coronary angiogram before major cardiac or non-cardiac surgeries to define coronary anatomy and optimise perioperative risk management.
6. Unexplained Cardiac Symptoms with High Risk Profile Patients with multiple cardiovascular risk factors and unexplained symptoms — particularly diabetics who experience silent ischemia — may be referred directly for coronary angiogram when the clinical suspicion is high.
Coronary Angiogram as a Coronary Artery Blockage Test: How It Detects Disease
The coronary angiogram functions as the definitive coronary artery blockage test by directly demonstrating the anatomy of the coronary circulation. Here is how blockages are detected:
During the procedure, a contrast dye (iodine-based radiopaque agent) is injected directly into the coronary arteries through a thin, flexible tube called a catheter. As the dye flows through the arteries, it absorbs X-rays and appears as a bright white stream on the fluoroscopy screen in the cathlab.
Healthy coronary arteries appear as smooth, continuous white channels with gradual tapering. Diseased arteries show:
- Stenosis (Narrowing): A localised narrowing of the vessel lumen, expressed as a percentage. A 70% stenosis means 70% of the vessel diameter is blocked by plaque.
- Occlusion (Complete Blockage): Abrupt termination of the contrast column where the artery is completely blocked.
- Diffuse Disease: Long segments of irregular, narrowed vessel indicating widespread atherosclerosis.
- Collaterals: Small compensatory vessels that develop to supply blood beyond a chronic blockage — an important finding that influences management decisions.
The cardiologist simultaneously records multiple angiographic projections from different angles to fully characterise each coronary artery lesion in three dimensions.
Coronary Angiogram in the Coronary Angiogram Cathlab: The Procedural Environment
The coronary angiogram cathlab is the specialised procedural room where all coronary angiography is performed. Understanding the cathlab environment reduces the intimidation many patients feel when they first enter this space.
The cathlab is equipped with:
- A motorised X-ray imaging system (C-arm) — a large, moveable X-ray unit that rotates around the patient to capture images from multiple angles
- High-resolution fluoroscopy monitors — real-time X-ray screens the cardiologist watches during the entire procedure
- A procedural table — a flat, narrow table that allows the C-arm to rotate freely around the patient
- Contrast injection systems — for delivering precisely controlled amounts of contrast dye
- Haemodynamic monitoring — continuous ECG, blood pressure, and oxygen saturation monitoring throughout the procedure
- Emergency resuscitation equipment — defibrillator, crash cart, and full cardiac life support availability
The cathlab team typically includes the interventional cardiologist performing the procedure, a trained cardiac cathlab technologist, a scrub nurse, and a circulating nurse.
Jayam Hrudayalaya operates a dedicated cathlab in Hosapete where coronary angiograms are performed by Dr. T. Sandeep, ensuring that every patient receives expert procedural care in a fully equipped, professionally managed interventional cardiology facility.
Coronary Angiogram Under Local Anaesthesia: What to Expect
One of the most common patient concerns is: will I be unconscious during the procedure? The answer, in virtually all standard coronary angiogram cases, is no.
A coronary angiogram under local anaesthesia is the standard approach. Here is what this means in practice:
You remain fully awake throughout the entire coronary angiogram procedure. The only area anaesthetised is the small puncture site — either the wrist (radial artery approach) or the groin (femoral artery approach) — where the catheter is inserted.
Local anaesthetic injection: A small amount of lignocaine (local anaesthetic) is injected under the skin at the puncture site. You will feel a brief sting from the injection — similar to a dental anaesthetic — after which the area becomes numb. The actual arterial puncture and catheter insertion are performed through this numbed area.
During the procedure: You will feel no pain from the catheter as it travels through the arteries toward the heart. The blood vessels have no pain nerve fibres, so catheter movement is not felt. You may experience:
- A brief warm or flushing sensation when contrast dye is injected — completely normal
- Mild pressure at the access site
- Brief palpitations during injection into specific arteries — normal and transient
Sedation: Mild intravenous sedation (anxiolysis) is sometimes given to patients who are highly anxious, but this is not general anaesthesia — you remain conscious and can communicate with the team throughout.
The use of coronary angiogram under local anaesthesia means faster recovery, elimination of general anaesthesia risks, and the ability to inform the cardiologist immediately if you experience any symptoms during the procedure.
The Complete Coronary Angiogram Procedure: Step by Step
Step 1 — Preparation and Consent
On the day of your coronary angiogram, you will be asked to fast for 4–6 hours before the procedure. An intravenous (IV) line is inserted in your arm for medication administration. You change into a hospital gown, and the cathlab team reviews your history, allergies, and current medications. Written informed consent is obtained.
Step 2 — Positioning and Monitoring
You lie flat on the cathlab procedural table. ECG electrodes are attached to your chest for continuous cardiac monitoring. Blood pressure cuff and pulse oximeter are connected. The cathlab team maintains sterile conditions throughout.
Step 3 — Access Site Preparation
The coronary angiogram access site — most commonly the radial artery at the wrist in modern practice — is cleaned and draped with sterile covers. Local anaesthetic is injected to numb the area completely.
Step 4 — Arterial Puncture and Sheath Insertion
A small puncture is made in the radial artery and a thin plastic tube called a sheath (typically 5–6 French in diameter — less than 2mm) is inserted. This sheath serves as the entry port for all subsequent catheters.
Step 5 — Catheter Navigation to the Heart
A long, thin, flexible catheter is passed through the sheath, into the artery, and navigated under X-ray guidance (fluoroscopy) up the arm, through the subclavian artery, into the aorta, and positioned at the opening of the coronary arteries. You will not feel this journey — blood vessels have no pain sensory fibres.
Step 6 — Contrast Injection and Image Acquisition
Contrast dye is injected through the catheter into each coronary artery in turn. Multiple projections (angiographic views from different angles) are recorded as the dye flows through the coronary circulation. The cardiologist rotates the C-arm imaging system to capture the anatomy from every clinically relevant angle.
Step 7 — Left Ventriculography (if required)
In some cases, contrast is also injected into the left ventricle to assess overall heart function (ejection fraction) and detect wall motion abnormalities.
Step 8 — Catheter Removal and Haemostasis
After complete image acquisition, the catheter is removed and the sheath is taken out. The access site is closed — for radial access, a compression band (TR Band) is applied to the wrist for 2–3 hours. For femoral access, manual compression or a vascular closure device is used.
Step 9 — Recovery
You are transferred to a recovery area where heart rate, blood pressure, and access site are monitored for 2–4 hours before discharge.
Total procedure time: The coronary angiogram itself typically takes 20 to 45 minutes for a standard diagnostic study.
Catheter Angiogram Risks: What Every Patient Should Know
The coronary angiogram is one of the safest invasive cardiac procedures available, but like all invasive investigations, catheter angiogram risks exist and must be discussed with every patient:
Minor Risks (Common, Self-Limiting):
- Bruising at the access site — very common with radial access; usually resolves within 1–2 weeks
- Allergic reaction to contrast dye — mild reactions (rash, itching) occur in approximately 1–2% of patients; premedication with antihistamines and steroids is given to patients with known dye allergies
- Transient drop in blood pressure — usually responds quickly to IV fluids
- Brief arrhythmias — typically self-terminating during contrast injection
Serious Risks (Rare):
- Stroke — approximately 0.1–0.2% risk
- Heart attack — extremely rare (< 0.1%) in a diagnostic angiogram
- Major bleeding at access site — rare with radial approach; requires intervention if it occurs
- Contrast-induced nephropathy — temporary worsening of kidney function in patients with pre-existing kidney disease; adequate hydration before and after the procedure significantly reduces this risk
- Arterial dissection or perforation — very rare complications manageable in the cathlab
Overall mortality risk from a diagnostic coronary angiogram in a stable patient is approximately 1 in 1,000 to 1 in 2,000 — making it an extremely safe procedure when properly indicated and performed by an experienced interventional cardiologist.
Heart Angiography Procedure India: Access, Cost, and Availability
The heart angiography procedure India has expanded significantly in availability, with dedicated cathlab facilities now present in major district hospitals and specialised cardiac centres across the country.
Approximate Coronary Angiogram Cost in India:
| Facility Type | Approximate Cost |
|---|---|
| Government Hospital | ₹0 – ₹5,000 |
| District Private Cardiac Hospital | ₹8,000 – ₹18,000 |
| Dedicated Cardiology Centre | ₹12,000 – ₹25,000 |
| Corporate / Tertiary Hospital | ₹25,000 – ₹50,000 |
For patients enrolled under PM-JAY (Ayushman Bharat), SAST (Karnataka), ESI, or other government BPL health schemes, the heart angiography procedure India at empanelled centres is covered at zero cost to the patient. All procedure costs — including cathlab charges, contrast dye, catheters, and cardiologist fees — are covered under the scheme package rate.
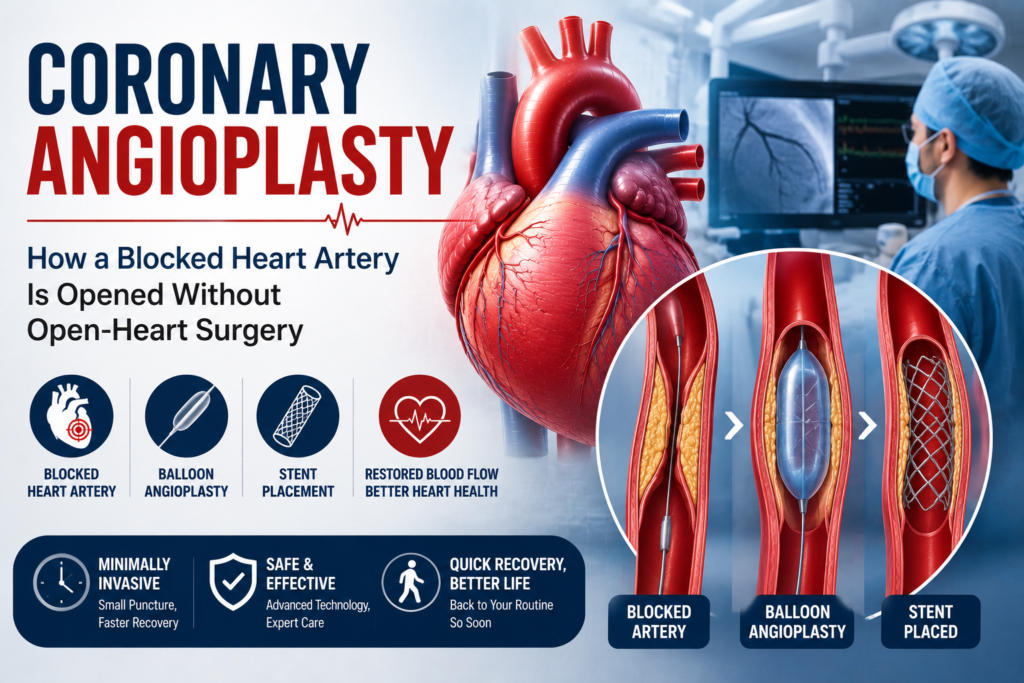
Angiogram vs Angioplasty Difference: Understanding the Critical Distinction
The most common source of confusion for patients referred for cardiac catheterisation is the angiogram vs angioplasty difference. These are two distinct procedures, although they are related and sometimes performed in the same session.
| Feature | Coronary Angiogram | Coronary Angioplasty (PTCA) |
|---|---|---|
| Purpose | Diagnostic — to see the arteries | Therapeutic — to open a blockage |
| What happens | Contrast dye injected; images taken | Balloon inflated + stent placed inside blocked artery |
| Duration | 20–45 minutes | 45 minutes – 2 hours |
| Decision | Always planned in advance | Planned or emergency |
| Result | Diagnosis only | Treatment of blockage |
| Stent used? | No | Yes (in most cases) |
| Recovery | Same-day or next-day discharge | 1–2 days hospitalisation |
In simple terms: the angiogram shows the problem; the angioplasty fixes it. When a significant blockage is found during a coronary angiogram, the cardiologist may proceed to angioplasty in the same session (ad hoc PCI) if the clinical situation is appropriate, or schedule it as a separate planned procedure.
Angiogram Results Interpretation: Understanding Your Coronary Angiogram Report
Angiogram results interpretation is the cardiologist’s most critical task after the images are acquired. Here is how to understand the key terminology in a coronary angiogram report:
Vessel Nomenclature:
- LAD (Left Anterior Descending) — supplies the front wall of the left ventricle; the most critical coronary artery
- LCX (Left Circumflex) — supplies the lateral and posterior walls
- RCA (Right Coronary Artery) — supplies the inferior wall and often the SA and AV nodes
Stenosis Grading:
| Stenosis Severity | Percentage Narrowing | Clinical Significance |
|---|---|---|
| Minimal | < 30% | No haemodynamic significance |
| Mild | 30–49% | Monitor; medical management |
| Moderate | 50–69% | Consider FFR assessment |
| Severe | 70–89% | Significant; likely needs intervention |
| Critical | 90–99% | Urgent intervention needed |
| Total Occlusion | 100% | Complete blockage — CTO |
Dominance:
Most people are right-dominant (RCA supplies the posterior descending artery). Approximately 10–15% are left-dominant. Dominance affects the significance of disease in specific vessels.
Common Diagnoses in Angiogram Reports:
- Normal coronary arteries — No obstructive disease; cardiac symptoms have another cause
- Single-vessel disease — One artery significantly narrowed; usually suitable for angioplasty
- Double-vessel disease — Two arteries significantly narrowed; intervention planned
- Triple-vessel disease — All three major arteries diseased; bypass surgery often preferred
- Left main stem disease — Critical blockage at the origin of the left coronary system; high-risk, requires urgent multidisciplinary decision
Angiogram Recovery Time: What to Expect After Your Procedure
Angiogram recovery time depends on the access site used and whether the procedure was purely diagnostic or included angioplasty.
After Radial Access (Wrist):
- A compression wrist band (TR Band) is applied immediately after the procedure and gradually deflated over 2–3 hours
- You can sit up, eat, and drink within 1–2 hours of returning to the recovery area
- Most patients are discharged the same day — typically 4–6 hours after the procedure
- Wrist soreness and bruising are common for 1–2 weeks; avoid heavy lifting with that arm for one week
- Driving should be avoided for 24 hours; light activities can resume from the next day
After Femoral Access (Groin):
- You must lie flat for 4–6 hours after the procedure to prevent bleeding
- Discharge typically occurs the next morning after overnight observation
- Avoid strenuous physical activity and heavy lifting for 5–7 days
- Report immediately if you notice expanding swelling, significant bleeding, or severe pain at the groin site
General Post-Angiogram Instructions:
- Drink plenty of water — 2–3 litres over the 24 hours following the procedure to help flush the contrast dye through the kidneys
- Take all prescribed medications as directed — antiplatelet drugs, statins, and any new prescriptions from your cardiologist
- Avoid submerging the access site in water (baths, swimming) for 48–72 hours; showering is permitted
- Attend all follow-up appointments as scheduled — your cardiologist will review the angiogram findings, discuss treatment options, and plan next steps
Coronary Angiogram: The Gateway to Life-Saving Treatment
The coronary angiogram is more than a diagnostic test — it is the gateway to precisely targeted, life-saving cardiac treatment. Once the cardiologist has a definitive map of the coronary circulation, every subsequent decision — whether to treat with medications alone, proceed to angioplasty and stenting, or recommend bypass surgery — is based on objective anatomical evidence rather than inference.
Patients who defer or avoid a recommended coronary angiogram out of fear or misunderstanding risk allowing treatable coronary artery disease to progress silently toward a major heart attack. The procedure itself, as this guide has demonstrated, is safe, minimally invasive, performed under local anaesthesia, and completed in under an hour.
Conclusion
The coronary angiogram is the definitive answer to the question every cardiac patient ultimately needs answered: are my heart arteries normal, or is there a blockage that needs treatment? No other single investigation provides the directness, accuracy, and actionable clarity of a coronary angiogram. If your cardiologist has recommended one, the information in this guide should reassure you that this is a safe, well-established procedure performed every day in cardiac centres across India — and that the knowledge it provides is indispensable for your cardiac care.
Your coronary arteries keep your heart alive. A coronary angiogram keeps your coronary arteries understood.